
Brian Schiff’s Blog
Injury Prevention, Sports Rehab & Performance Training Expert
 0
0
I must admit that I am always looking for new ways or tools to enhance my practice and work as a sports physical therapist. I recently completed the necessary hours of training to perform dry needling in the state of North Carolina. I trained with Myopain Seminars and have nothing but great things to say about their courses.
For those unfamiliar with trigger point dry needling (TDN), it is a treatment gaining traction in the therapy world. Dry needling is a treatment that involves a very thin needle being pushed through the skin to stimulate a trigger point. Dry needling may release the tight muscle bands associated with trigger points and lead to decreased pain and improved function for those suffering from pain related to muscular dysfunction.
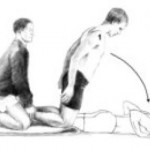
Trigger points may ultimately refer pain to other sites, and research indicates that TDN can reduce acidity in the muscle and clear out pain propagating chemicals. The picture below is an example of me performing trigger point dry needling to the upper trapezius of a 16 y/o female.

This particular client had been suffering from an inability to lift the arm above shoulder height and marked shoulder pain since September 2013. She also mentioned having headaches at school. Clinically, she was diagnosed with multi-directional instability and scapular dyskinesis by the referring MD. We began working on a scapular stabilizer and rotator cuff strengthening program in late November that was helping to diminish pain and increase function. However, she continued to c/o pain in school, stiffness and headaches.
Obviously I am a BIG fan of bodyweight training and incorporate it into many of my fitness and rehab programs. to that end, I wanted to let you know about a great bodyweight training bundle being released today. I was asked to contribute to this product bundle and have added my very own Ultimate Rotator Cuff Training Guide ($39.95 value).
The bundle has something for everyone looking to:
- Burn more fat
- Build more muscle
- Increase overall fitness
It features all of the following:
- 8 Bodyweight Muscle Building ebooks
- 6 Bodyweight Fatloss ebooks
- 5 Bodyweight Play/Trick ebooks
- 10 Bodyweight Video/Workout Programs
- 5 Nutrition/Recipe ebooks
- 4 Bodyweight Flexibility/Rehab Programs
Click the image below for more information. Act now to get all these resources at a steep discount!

The shoulder mobility screen in the FMS often reveals side-to-side asymmetries. It is more common to see hypermobility in female clientele, while their male counterparts exhibit more hypomobility. Overhead athletes tend to demonstrate excessive horizontal external rotation and a relative loss of internal rotation on the dominant side. This hypomobility can be detrimental to overhead athletes and increase risk for overuse injuries if it becomes excessive.
The following exercise is an effective way to improve shoulder mobility and optimize function. One important point is to focus on form and move very deliberately through the motion.




Execution: Begin lying on the floor face up. Bend the left knee up to 90 degrees and cross the right leg over top of the left interlocking them. Roll to the left side and pin a folded towel or pad between the right knee and the floor. Place the arms in 90 degrees of shoulder flexion with the right on top of the left in an outstretched position. Next, slowly sweep the right arm up overhead and around the body as you attempt to place the torso/back on the floor. The finish position for the right arm will be reaching the right hand and arm up behind the back.
Exhale as you perform the sweeping motion and hold the end position for 2 seconds. Reverse direction and return to the start position. Perform 5-10 repetitions on each side.
Application: Limited shoulder mobility is a common finding, especially among male clientele with tightness in the pecs, lats and posterior shoulder. Asymmetry with respect to mobility is common with greater difficulty found trying to reach the dominant arm up behind the back on the FMS shoulder mobility screen. This exercise will help improve thoracic spine motion and shoulder mobility. The focus should be on strict form and proper stabilization to avoid unwanted motion. Pinning the pad (or towel roll) to the floor will help ensure better stabilization.
If hypomibility is an issue and clients score a 1, foam rolling the pec minor/major, latissimus dorsi and the posterior rotator cuff musculature prior to performing the exercise will be helpful. Stability training can be added in later once the soft tissue mobility restrictions and movement pattern is improving.
One of the most difficult problems to treat in the clinic is chronic pain related to tendinopathy. More specifically, the Achilles tendon, patella tendon and elbow extensors often present challenges for doctors and clinicians alike when it comes to effectively reducing or resolving pain. Over time, people develop chronic inflammation or even little tears in the muscles running up to the lateral epicondyle.

There have been many studies done looking at PRP over the past 5-10 years. The debate continues, however, with respect to its efficacy in terms of results, especially given the fact that patients must currently pay out of pocket for the procedure. I have written two earlier posts on PRP that you may be interested in reading as a back drop for this one:
2011 – An Update on Platelet Rich Plasma
2011 – Platelet Rich Plasma and Rotator Cuff Repairs
Currently, my approach to treating these injuries involves an approach focused on soft tissue mobilization via instrument assisted soft tissue mobilization, stretching, strengthening and a trial of iontophoresis in most cases. We also offer dry needling at our facility and this has been effective in reducing pain. I will talk more about this point later as it relates to the prospective multi-center trial summarized by Mishra et al. in the February 2014 edition of the American Journal of Sports Medicine.
Before I get to the study, I thought it would be pertinent to provide some straightforward information on PRP as it is a question that comes up with patients on a regular basis. Essentially, the process is as follows:
1. Collect 30-60 ml of blood form the patient’s arm
2. Blood is then placed in a centrifuge. The centrifuge spins and separates the platelets from the rest of the blood.
3. A syringe is then used to extract 3-6ml of the platelet-rich plasma
4. The concentrated platelets are then injected into the elbow (or site being treated)

The thought behind PRP is to increase the growth factors up to 8x, which promotes temporary relief and stops inflammation. The question is how successful and cost effective is this process? Consider that opting for surgery will run between $10,000 and $12,000 figuring in costs for the surgeon, hospital/surgery center, anaesthesiologist, etc. PRP injections will cost upwards of $1000, so one would think that would be a favorable option for insurers if surgery could be averted.
What about cortisone injections? They are widely used as a survey of 400 members of the American Academy or Orthopedic Surgeons found that 93% had administered a corticosteroid injection for lateral epicondylar tendinopathy. According to Bisset et al (Br Med J 2006) and Lindhovius et al (J Hand Surg Am 2008) cortisone injections do provide short term pain improvements but also result in a high rate of symptom recurrence. There are other potentially harmful side effects from injections including: reduced collagen synthesis, depletion of human stem cells, depigmentation, and enhancement of fatty and cartilage like tissue changes that can lead to tendon ruptures.
So, the big question is whether or not tendon needling with PRP is an effective treatment option for chronic tennis elbow suffers. Mishra and his colleagues set out to examine this with a double blind, prospective, multi-center randomized controlled trial of 230 patients. In the study, the patients were teated at 12 different facilities over 5 years. All patients had at least 3 months of pain/symptoms and failed conservative treatment.
Perhaps one of the most researched topics is ACL injuries. I have been studying and working for years in my clinical practice to find the best ways to rehab athletes following injury as well as implement the most effective injury prevention strategies. Prior studies indicate prevention programs even when self directed can be successful.
However, on the whole injury rates have not declined over the past decade or so. Much attention has been given to valgus landing mechanics, poor muscle firing, stiff landings, genetic difference between males and females, ligament dominance, quad dominance, and so forth. The predominant thoughts today for prevention center around neuromuscular training and eliminating faulty movement patterns (refer to work being done by Timothy Hewett and Darin Padua).
We also know from a biomechanical standpoint that the hamstrings play an integral role in preventing excess anterior tibial translation, and as such hamstring strengthening needs to be a big part of the rehab and prevention program. I believe in hamstring training that allows for activation in non-weaightbearing and weight bearing positions. Common exercises I will use include:
- HS bridging patterns (double /single leg, marching, knee extension, stability ball)
- Nordic HS curls
- HS curls (stability ball, TRX or machine)
- Sliders – focus on slow eccentric motion moving into knee extension followed by simultaneous curls/bridge
- Single leg RDL (add dumbbells or kettle bells for more load)


Note: click on any of the thumbnail images above for a full view of the exercise. From left to right: Nordic HS curls, sliding hamstring curls and single leg RDL).
A recent blog post entry by the UNC Department of Exercise and Sport Science (@UNCEXSS) has spurred my post today. Click here to read their entry on optimizing injury prevention based on work done by Professor Troy Blackburn regarding the effect of isometric and isotonic training on hamstring stiffness and ACL loading mechanisms. The research that was done holds promise for hamstring training designed to increased musculotendinous stiffness (MTS).
 Back to top
Back to top